
Karamoja leads the way: Why integrated malaria prevention is Uganda’s smart move in the fight against malaria
by Daudi Ochieng
Approx reading time:
“If you do a random spot check on malaria trends during the SMC period, you see fewer children getting sick. Now, with the malaria vaccine, we anticipate even better results.” — Dr James Lemukol, District Health Officer, Moroto district.
In Karamoja — one of Uganda’s most malaria-burdened subregions — a critical shift is underway. Health leaders, district officials and implementing partners gathered in Moroto in May 2025 to align on a bold, evidence-driven approach: integrating seasonal malaria chemoprevention (SMC) with the newly introduced malaria vaccine (R21), which targets children between the ages of six months and five years old. The vaccine boosts the child’s immune system to recognise and attack malaria, while helping to stop the disease before it becomes severe or deadly.
Why integration now?
Uganda is rolling out the malaria vaccine in 105 high-transmission districts, targeting over one million infants. Meanwhile, SMC — implemented in Karamoja since 2021 — has significantly reduced malaria cases among children under five. But in Karamoja, these interventions, when implemented in isolation, risk missed opportunities and fragmented coverage.
Evidence from Mali and Burkina Faso has highlighted the power of integration. Leveraging the SMC programme with the malaria vaccine could reduce clinical malaria by 63 percent and severe malaria by 70 percent — outperforming either intervention used on its own. Depending on the context, it may not always be feasible, effective or cost-effective to integrate services. But, where the research points to greater impact, we need to act. That’s why Uganda is taking this evidence from the page to the field.
“We should be actively seeking opportunities to reduce the cost per child and integrate services wherever possible,” noted Dr Anthony Nuwa, Malaria Consortium’s Senior Country Technical Coordinator. “Karamoja already has one of the most versatile community health systems in Africa — our village health teams (VHTs) deliver both integrated community case management (iCCM) and SMC. This is the model to build on.”
Working smarter with fewer resources
Integration is not just about administrating drugs or coordinating calendars. It is about optimising every available resource — from efficient use of VHTs’ time to cold chain logistics — in a setting where funding is increasingly uncertain.
“We live in unprecedented times”, said Dr Stephen Legesi Pande, Director of Moroto Regional Referral Hospital. “We must use what we have more wisely.”
That’s why integration was a key theme of the Moroto engagement — and why Uganda’s Ministry of Health, in partnership with the World Health Organization, Gavi, UNICEF and Malaria Consortium among others, fully support the approach.
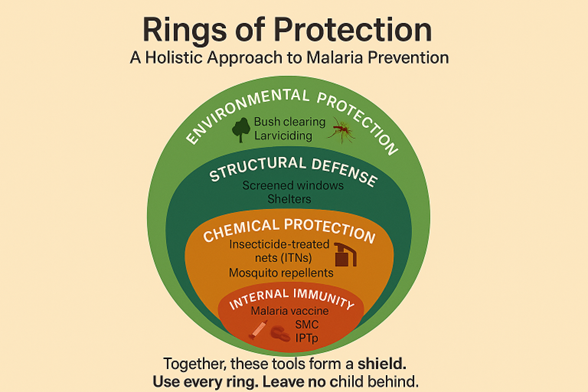
The “Rings of Protection” framework illustrates Uganda’s integrated approach to malaria prevention — combining environmental control, housing improvements, chemical protection, personal use of insecticide-treated nets (ITNs) and repellents, and internal immunity through SMC, intermittent preventive treatment for pregnant women (IPTp) and the malaria vaccine. When layered together, these interventions form a powerful shield against malaria.
“Let’s not despair,” urged Dr Jimmy Opigo, Commissioner for Uganda’s National Malaria Elimination Division (NMED). “This vaccine is part of our future. But it must be included alongside long-lasting insecticidal nets and SMC — as part of the shield.”
When systems work together, everyone wins
At a high-level engagement meeting in Moroto in May 2025, local government, regional health leaders and national policymakers reaffirmed their commitment to integration. The rationale was straightforward: leveraging delivery platforms can reduce missed opportunities, enhance coverage and optimises scarce resources in Uganda.
According to an internal report from Malaria Consortium’s regional engagement in Karamoja in May this year, 97 percent of surveyed caregivers believe that SMC prevents severe malaria. With such a high level of trust, leveraging the familiar SMC delivery system to roll out the malaria vaccine makes strategic sense.
How integration works in practice
The integration of the malaria vaccine with SMC builds on an established, trusted delivery system. During the door-to-door distribution of SMC, VHTs also identify children who have not received any or all of their routine immunisations (known as ‘zero-dose’) — including the malaria vaccine — and refer them to the nearest public health facility. This linkage ensures that zero-dose or partially vaccinated children are not left behind. The malaria vaccine is administered in four doses: the first three are given one month apart between the ages of 6 and 11 months, with the final booster dose delivered six months after the third dose. By synchronising SMC visits with immunisation referral, Uganda is creating a more efficient and equitable pathway to full malaria protection.
In Togo, Malaria Consortium and the National Malaria Control Programme are implementing the Zero-dose project in 21 districts as of 2024. SMC community distributors have been trained to check children’s vaccination status for preventable childhood diseases — including the pentavalent vaccine, which protects against diphtheria, tetanus, pertussis, hepatitis B and Haemophilus influenzae type b — and to refer those who have missed doses to a nearby vaccination centre. This includes sharing information about children identified with health facility managers, so they can plan outreach for communities with low vaccination uptake.
“After two doses, a child is still vulnerable”, noted Dr Possy Mugyenyi, Uganda National Expanded Programme on Immunization Advisor. “We must ensure full completion — and that means making it easier for caregivers to say yes.”
Leaders across the region, including Kotido District Chairman Mr Lotee Paul Komol, pledged their full political support: “We’ve seen fewer outpatient cases. We will support this new intervention and preserve these gains.”
The takeaway
Malaria is multi-faceted — and no single intervention can win this fight alone. Integration is more than just technical alignment. It’s a signal of resilience, equity and trust. It ensures that no child is left behind, no dose wasted and no health worker overstretched. It is also a strategic response to shrinking global health funding: smarter, cost-effective use of logistics, community health platforms and human resources.
Karamoja has shown what is possible when political leadership, community trust and technical innovation converge. As the region leads the way, Uganda is poised to set a powerful example for the continent: that integration is more than just strategy — it’s survival.
Now is the time to scale.
Malaria Consortium calls on national policymakers, implementing partners and funders to align behind an integrated malaria prevention strategy — one that leverages existing systems, reduces missed children and accelerates Uganda’s path to malaria elimination.
Read more about Malaria Consortium’s SMC programme