South Sudan: strengthening capacity for improved monitoring and evaluation
Background
Malaria is endemic in tropical climates, especially in sub-Saharan Africa. When cases of malaria are presented at health facilities, particularly at primary health care units in South Sudan, it is largely diagnosed on clinical grounds alone, with fever cases assumed to be malaria. This leads to an over-diagnosis of malaria and the irrational use of antimalarial drugs, which can result in drug stock-outs during critical times of the year as well as the development of drug resistance. This leads to high morbidity and mortality despite efforts by the government and partners to treat, prevent and control malaria every year.
As the world’s youngest nation, South Sudan is also among the poorest. With an estimated population of 11.8 million in 2013, many are internally displaced as a result of the current conflict, while others have had to flee the country.
The health burden
The Health Sector Development Plan (HSDP 2012 - 2016) guides all priority health interventions in the country. According to HSDP, only 44 percent of the population lives within a five kilometre radius of a functioning health facility, and the average use of these facilities per capita is estimated at only 0.2 visits per year. Only one of five people use a healthcare facility in a year. National reports have proven that children under five years are the most vulnerable, accounting for 40 percent of the total reported cases – mainly caused by malaria, pneumonia, diarrhoea and malnutrition.
The Ministry of Health faces major challenges in controlling malaria, which is among the leading causes of morbidity and mortality. The result is a failure to meet nearly all the targets for the Millennium Development Goals. The infant and child mortality rates have remained staggeringly high at 102 per 1,000 live births and 135 per 1000 live births, respectively.
Our response
Through its integrated community case management (iCCM) approach, Malaria Consortium has been providing community services that address these conditions by reaching out to communities and households in Aweil West and Aweil Centre Counties of Northern Bahr el Ghazal State. Based on the primary healthcare institutions’ reports, a decline of morbidity and mortality as a result of these conditions can be seen since Malaria Consortium initiated its iCCM and nutrition projects, with funding from UK aid from the UK government.
Malaria Consortium has supported the placement of a senior technical advisor to the National Malaria Control Programme, who supports in policy development and establishing health management information systems through capacity building for quality diagnosis and management of malaria. Continued support for iCCM and nutrition has bridged the gap in supporting the National Malaria Strategic Plan surveys and built systems and mechanisms that promote sustainability and have ensured community ownership.
Efforts in South Sudan for the past three years have culminated in the launch of the National Malaria Strategy, the National Monitoring and Evaluation Plan, and state action plans for monitoring and evaluation.
backRelated resources
 Resource: Project
Resource: ProjectPublished 9 January 2017
Positive Deviance - an innovative approach to improve malaria outcomes in Myanmar
 Resource: Poster
Resource: PosterPublished 31 March 2016
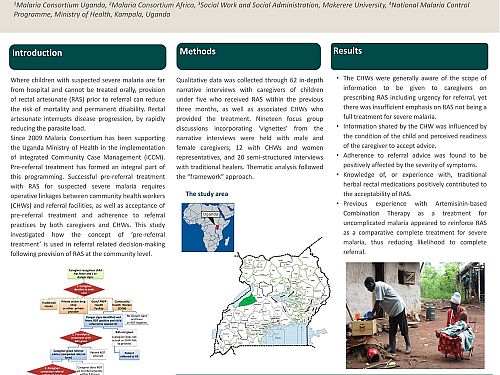
Community level understanding of the concept of pre-referral treatment and impact on referral-related decision-making following provision of rectal artesunate. A qualitative study in Western Uganda
 Resource: Training materials
Resource: Training materialsPublished 31 March 2016
Guide to developing and monitoring a research uptake plan
 Resource: Project brief
Resource: Project briefPublished 21 September 2015
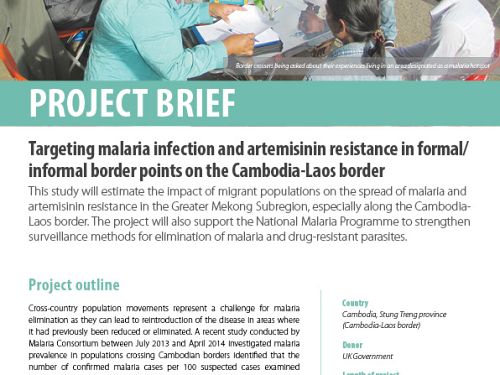
Targeting malaria infection and artemisinin resistance at formal and informal border points on the Cambodia-Laos border
 Resource: Technical brief
Resource: Technical briefPublished 18 May 2015
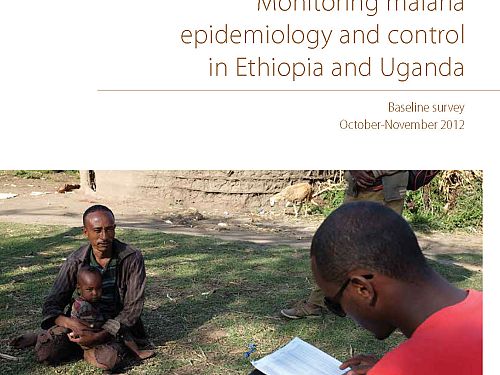
Monitoring malaria epidemiology and control in Ethiopia and Uganda: Baseline survey
 Resource: Project
Resource: ProjectPublished 24 February 2014
Positive Deviance - an innovative approach to improve malaria outcomes in Myanmar
 Resource: Project brief
Resource: Project briefPublished 1 January 2014
Positive deviance pilot
 Resource: Project brief
Resource: Project briefPublished 18 November 2013
iCCM guidelines and implementation framework