
Generating logistics data for decision-making and accountability within SMC campaigns in Nigeria
23 April 2017While contributing to the reduction of malaria during the rainy season in the Sahel, the UNITAID-funded ACCESS-SMC project has also invested in strengthening health systems in Burkina Faso, Chad, Guinea, Mali, Niger, Nigeria and The Gambia. One example is the improvement of logistics management information systems (LMIS), which collect, organize and present logistics data for programmatic decision making and enable accountability by the project and participating countries for donated SMC treatments.
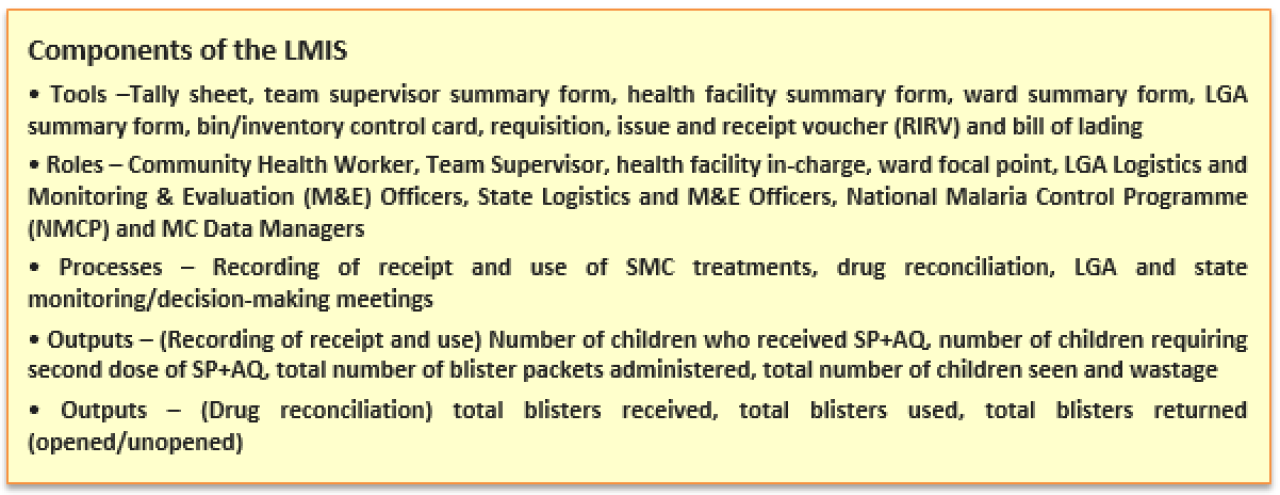
In Nigeria, with support from Management Sciences for Health (MSH) and Malaria Consortium (MC), a systematic process was used to attain, maintain and continually improve a functional, manual LMIS as a component of the SMC campaign. Nigeria’s LMIS provides information for decision making and accountability at many levels - community, health facility, local government area (LGA) and state - before during and after SMC campaigns.
Understanding the flow of SMC commodities was integral to designing the LMIS. In Nigeria, SMC treatments procured through the ACCESS-SMC project were first cleared from the port and delivered to Central Medical Stores (CMS) in Sokoto and Zamfara States for storage. A few days before the five-day distribution cycle began, treatments were distributed by each CMS to selected hub facilities within target LGAs. On the morning of the first day of each cycle, treatments are collected by a Team Supervisor and distributed to CHW teams. These teams then would administer treatments in communities to children under five who are eligible to receive the treatment.
To determine what logistics information should be collected, the design team had to decide what outputs they would like the LMIS to provide and how campaign managers would use the information to achieve mid-term results. It was agreed that information from the LMIS would be used to a) ensure there was an uninterrupted supply of treatments to CHWs on each day of the four cycles in an SMC campaign round, b) avert stock-outs or over-stocks of treatments by CHW teams, c) understand how many treatments were administered to eligible children per cycle, d) know what volumes of treatment stocks were used/wasted/lost/left over e) identify trends in consumption and f) provide insight around the expected correlation between services and logistics data. Thus, the logistics data essential to identifying the information needs were stock-on-hand, consumption data, losses and adjustments.

Other critical data elements were beginning balances, quantity received, quantity withdrawn, quantity expired and quantity required for re-supply.
After two years of using LMIS during SMC campaigns in Nigeria, three key lessons were learned. First, while the LMIS collects and reports the essential data items for logistics management, real-time use of data for decision-making, which is very useful during a high intensity distribution campaign like this, was difficult because the LMIS system is a manual system with repeat summarization of the same data at five levels within the space of four hours. Second, the LMIS collects vast amounts of data, and there is more data being collected and managed than is needed to answer key questions at different levels of the system. Third, there were quality issues associated with collecting data. Data completeness, timeliness, accuracy and accessibility all tend to be sub-optimal. Reasons for this include:
- The fast pace of the campaigns results in CHWs and Team Supervisors being under pressure to meet their daily targets for administration of treatments. Coverage data is prioritized over drug accountability data.
- Distances from community distribution points to where the Team Supervisors were located were quite far, therefore, reconciliation between CHW teams and Team Supervisors was done in a hurry, summarized over the phone or sometimes not at all.
- Reporting procedures were not followed correctly across the board, also due to specific skills gaps at the CHWs level.
- Supervision of data recording and management was insufficient due to funding limitations.
- Managers were not using the data for decision-making and so there was inadequate feedback to lower levels about their performance and no real motivation for improved data quality.
Some proposals for improving Nigeria’s LMIS are the automation of data collection, summarization, analysis and reporting, and a review of the indicators and information needed at different level of logistics management. The first would go a long way in providing real-time data that can be used for decision-making and accountability. If the system were to operate automatically at the Team Supervisor’s level this would decrease the overwhelming data management and manipulation burden. Also, having a clear focus on the collection of strategic information will ultimately help limit the collection of superfluous information. By improving the recording and transmission of relevant information through LMIS from lessons learned over the past two years, we can continue to strengthen the procurement and supply chain management capacity for the delivery of SMC to ensure all eligible children are reached.
Latest news
- International summit calls for AMR accountability in public health interventions21st March 2024
- Global SMC community celebrates new milestone at SMC Alliance Annual Meeting in Nigeria6th March 2024
- Scaling up key interventions could halve pneumonia-related childhood mortality13th February 2024
- Malaria Consortium and eGov Foundation join Mozambique’s national malaria programme to digitalise seasonal malaria chemoprevention campaigns8th February 2024
- World’s first malaria vaccine rollout launched in Cameroon22nd January 2024
- Digital solutions driving equitable access to health6th December 2023